
There’s a lot of misinformation floating around about Alzheimer’s disease, and sometimes it feels like you need to be a neuroscientist to sort through it all. This article will give you a brief primer on this disease and help you to understand the basics.
Discovery

A portrait of Dr. Alois Alzheimer
In the year 1906, Dr. Alois Alzheimer took the stage at a meeting of German psychiatrists to present his findings on “a peculiar disease.” An fifty-year-old patient named Auguste D. had come to Dr. Alzheimer experiencing memory loss, paranoia, personality changes, and difficulty sleeping. He was baffled by her symptoms and could do little to help her. Following Auguste’s death five years later, Dr. Alzheimer performed an autopsy on her brain and discovered that it was greatly shrunken in volume. Closer inspection revealed that Auguste’s brain was full of abnormal protein deposits located in and around the neurons. Dr. Alzheimer concluded that the pathology of her brain had caused his patient’s symptoms, a revolutionary idea at a time when mind was seen as completely separate from the physical body.
To Dr. Alzheimer’s dismay, the other physicians at the conference seemed uninterested in the findings–it’s said that they were anxious to hear the next speaker, who was to discuss “compulsive masturbation,” and as a result paid little attention to Dr. Alzheimer. When he died in 1915, he had no idea of the enormity of his discovery, or that a century later the disease bearing his name becoming the sixth leading cause of death in the U.S. Amazingly, had his patient Auguste been alive today, we could do no more to slow the progression of her disease than Dr. Alzheimer could more than a hundred years ago (see Where’s our cure to Alzheimer’s disease?).
Symptoms
Alzheimer’s disease has many symptoms aside from the well-known progressive memory loss. Personality and mood changes, such as depression and apathy, are common. Many patients experience reduced executive function, a broad category of cognition which includes attention, self-control, and problem solving. As the disease progresses, motor problems can appear, especially difficulty with speaking, swallowing, and walking. On average, patients with Alzheimer’s pass away within 4 to 8 years of diagnosis. The direct cause of death is often aspiration pneumonia, an infection of the lungs caused by food being improperly swallowed into the windpipe rather than the esophagus. Other common complications include bedsores, falls, urinary tract infection, malnutrition, dehydration, and organ failure.
In Our Brains
Some areas of the brain are affected more than others by this disease. Two areas of the brain that undergo particularly high levels of atrophy (i.e., tissue death) are the hippocampus and the entorhinal cortex. These two regions are most associated with declarative memory. Declarative memories are things that you can describe out loud, such as personal experiences or factual information. Conversely, procedural memory, also known as “muscle memory,” is the unconscious kind of memory that allows you to tie your shoes or play the piano. Interestingly, since procedural memory is handled by different brain systems, it is largely spared by Alzheimer’s disease. In other words, the inability of these patients to do basic tasks like dressing themselves is likely due to disruptions in motor function, and not from forgetting how to do so.
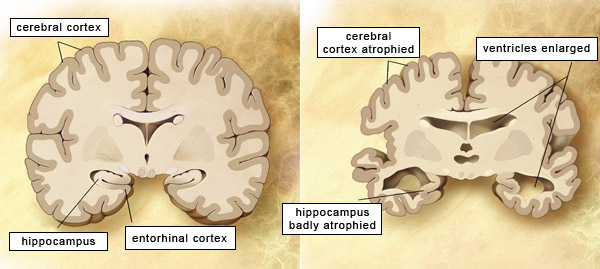
The left panel shows a cross-section of a healthy brain, while the right panels shows a brain with advanced Alzheimer’s disease. The hippocampus and entorhinal cortex are the brain regions most affected by this disease.
In addition to the hippocampus and entorhinal cortex, Alzheimer’s causes atrophy in various other brain regions involved with vision, mood, stress, language, movement, and proprioception (the sense of our body’s position in three dimensions, which is important for movement and coordination).
In Our Cells

Amyloid plaques and tau tangles inside the brain of an Alzheimer’s patient. Source
When Dr. Alzheimer examined his patient’s brain, he characterized the protein deposits into two types: those inside the neurons and those outside the neurons. The protein deposits inside neurons are known today as neurofibrillary tangles. They’re made of a protein called tau. When tau becomes hyperphosphorylated, meaning it has a large number phosphate groups attached to it, it becomes “sticky” and begins to adhere to other tau molecules. The protein deposits outside of neurons are called senile plaques, which are made of the amyloid beta protein. Like tau, amyloid beta can stick to itself to form large clumps in the brain. Both tangles and plaques are toxic to neurons in high concentrations, and are believed to be some of the main drivers of the disease’s progression.
In Our Genes
The genetic factors involved with Alzheimer’s disease is a very complicated topic (see The Genetics of Alzheimer’s Disease for a more detailed look). However, a brief overview will suffice for the purposes of this article. Alzheimer’s is typically classified into two types: familial, a rarer form that usually affects people younger than 65, and sporadic, which affects older patients and accounts for around 95% of Alzheimer’s diagnoses. Familial Alzheimer’s usually results from one of three genetic mutations: APP, which encodes a protein that is the precursor to amyloid beta; and PSEN1 and PSEN2, which encode an enzyme that helps turn APP into amyloid beta. These genes are highly penetrant, meaning that if you have one it’s very likely that you will develop familial Alzheimer’s disease. Additionally, a person who has one of these genes has a 50% chance of passing it on to each of their children.
The causes of of sporadic Alzheimer’s disease are more complicated. One gene that we know to be involved is APOE4. One copy of this gene increases your chances of getting the disease by about 2 to 3 times, while two copies increases your risk by nearly 15 times. This gene is actually fairly common, with 1 in 5 people possessing at least one copy. Many of these people never develop Alzheimer’s, and not all people with sporadic Alzheimer’s have APOE4. This tells us that other factors, which may be genetic or environmental, must also be involved.

Nearly 15% of the U.S. population has two copies of the APOE4 variant. Source
Learn More
Now that you’ve learned some basics about Alzheimer’s disease, here are some more articles for you to read and learn more:
- The Genetics of Alzheimer’s disease
- How to Reduce Your Dementia Risk in 2018
- Could We Ever Bring Back Alzheimer’s Patients Memories?
- Where’s our cure to Alzheimer’s disease?
References
n.a. What APOE means for your health. Alzheimer’s Drug Discovery Foundation. n.d. http://alzdiscovery.org/cognitive-vitality/what-apoe-means-for-your-health
Alzheimer’s Association. 2016 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2016;12(4):459-509.
Herrup, K. The case for rejecting the amyloid cascade hypothesis. Nature Neuroscience. 2-15;18(6):794-799.
Hippius H, Neundörfer G. The discovery of Alzheimer’s disease. Dialogues in Clinical Neuroscience. 2003;5(1):101-108.
Hirono, N., et al. Procedural memory in patients with mild Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders. 1997;8(4):210-216.
Leonard, W. Alzheimer’s Disease Complications. Healthline. 2014. https://owl.english.purdue.edu/owl/resource/560/10/

Pingback: There’s a New Drug for Alzheimer’s Disease… But Scientists Aren’t Celebrating. | AlzScience
Pingback: New Type of Brain Immune Cell Implicated in Alzheimer’s Disease | AlzScience
Pingback: Saliva Test for Alzheimer’s Disease Shows Encouraging Results | AlzScience
Pingback: Dementia Parents’ Awareness of their Own Illness May Predict Cognitive Decline | AlzScience
Pingback: Amyloid-Beta: Villain or Hero in Alzheimer’s Disease? (Podcast) | AlzScience
Pingback: Amyloid Beta: Villain, or Hero in Alzheimer's Disease?
Pingback: Episode 11: Maya Gosztyla -Alzheimers, Axons, Fruit Flies, and Free Time
Pingback: Macular Degeneration: Alzheimer’s Disease of the Eye? | AlzScience